Last week aku dpt berita anak kwn kakak da mengidap penyakit SLE @ Systemic Lupus Erythematosus..pada mulanya..Dr. kata dia kena Canser Darah...esoknya..confirm dia kena SLE..stakat ni..aku da dgr 3 org yg aku tahu kena penyakit ni..ttb rasa takut..takutt sgt2...dan aku mula mencari..seba skit mngenai penyakit ni..so..aku nak share ngn korg sume...mudah2an kita dan keluarga kita terhindar dari penyakit yg pasni membawa maut ini...
Apakah SLE?
Systemic Lupus Erythematosus (SLE) adalah penyakit kronik auto-imun di mana badan pesakit menghasilkan protein darah dengan banyaknya. Protin darah yang dipanggil antibodi ini dengan sendirinya memberi tindak balas terhadap tisu seseorang. Punca penyakit SLE tidak diketahui.
Sejarah
Lupus ialah perkataan Latin bagi serigala. Erythematosus bererti ruam merah. Pada tahun 1851, Dr. Cazenave telah menjumpai ruam merah di muka seorang pesakit yang kelihatan seperti gigitan serigala. Beliau telah menamakan ruam berkenaan Discord Lupus Erythematosus (DLE).
Pada tahun 1885, Sir William Osler telah mengenalpasti bahawa ramai orang yang mengidap lupus mempunyai penyakit yang bukan sahaja melibatkan kulit tetapi turut melibatkan organ dan sistem lain. Beliau telah menamakan penyakit tersebut Systemic Lupus Erythematosus (SLE).
Jenis-jenis Lupus
Discoid Lupus Erythematous (DLE)
•Hanya melibatkan kulit
•Jarang merebak ke organ lain
Systemic Lupus Erythematosus (SLE)
•Boleh merebak ke organ lain
•Boleh mengakibatkan kematian
Statistik
Lebih kurang 90% pengidap SLE adalah wanita sementara 10% adalah lelaki dan kanak-kanak.
Lebih kurang 90% wanita yang mengidap SLE berada di dalam lingkungan umur boleh hamil iaitu di antara 15 hingga 50 tahun.
Ratio pengidap SLE:
Di Barat, di kalangan Afro-Caribbeans – 1 dalam 250 –500 orang
Di Amerika Syarikat – 1 dalam 2,000 orang
Di negara China – 1 dalam 1,000 orang
Di Malaysia dianggarkan lebih daripada 10,000 orang telah disahkan mengidap SLE dalam jangka masa 30 tahun kebelakangan ini. Namun demikian, PSLEM percaya ada ramai lagi mereka yang mengidap SLE yang belum disahkan.
So many people have had comments like, "I had no idea Susan was so sick." That was because Susan did not want anybody to know.
Because lupus is such a crafty disease and flies under the general public's radar, this is a good opportunity to clear things up.
Lupus is an autoimmune disease, not an infectious disease like HIV. People with lupus have an overactive immune system. The body's defenses actually attack healthy tissue. This has been happening to Susan for 30 years or more.
She was diagnosed around 1990, but she had symptoms way before then. Originally, the disease would manifest itself as flu-like symptoms for about three weeks out of every three months, with fatigue extending a month after every flare-up.
In 2000, lupus attacked her central nervous system and involved her brain. The original result of this new development was pain. From late in January 2000 until the day before she died, she was in pain. On the scale of 1 to 10, there was no day that she didn't feel pain on an 8 to 10 level. (With 10 being all-encompassing.)
Lupus attacked her lungs, causing shortness of breath, sleeping problems, and more pain in the form of pleurisy. In addition to Hashimoto's thyroiditis (causing cold extremities) and Sjogren's syndrome (extremely dry eyes) and a few more isms that I have forgotten, life was getting difficult.
Top Searched Lupus Terms:
lupus disease, skin, rash, butterfly rash, lupus myositis, kidney disease, treatment, genetic, anticoagulant, diet, hereditary, discoid lupus, diagnosis, statistics, women, symptoms, contagious, lupus nephritis
What is lupus? What are the types of lupus?
Lupus is an autoimmune disease characterized by acute and chronic inflammation of various tissues of the body. Autoimmune diseases are illnesses that occur when the body's tissues are attacked by its own immune system. The immune system is a complex system within the body that is designed to fight infectious agents, such as bacteria and other foreign microbes. One of the ways that the immune system fights infections is by producing antibodies that bind to the microbes. People with lupus produce abnormal antibodies in their blood that target tissues within their own body rather than foreign infectious agents. Because the antibodies and accompanying cells of inflammation can affect tissues anywhere in the body, lupus has the potential to affect a variety of areas. Sometimes lupus can cause disease of the skin, heart, lungs, kidneys, joints, and/or nervous system. When only the skin is involved, the condition is called lupus dermatitis or cutaneous lupus erythematosus. A form of lupus dermatitis that can be isolated to the skin, without internal disease, is called discoid lupus. When internal organs are involved, the condition is referred to as systemic lupus erythematosus (SLE).
Both discoid and systemic lupus are more common in women than men (about eight times more common). The disease can affect all ages but most commonly begins from 20-45 years of age. Statistics demonstrate that lupus is somewhat more frequent in African Americans and people of Chinese and Japanese descent.
What causes lupus? Is it hereditary?
The precise reason for the abnormal autoimmunity that causes lupus is not known. Inherited genes, viruses, ultraviolet light, and certain medications may all play some role.
Genetic factors increase the tendency of developing autoimmune diseases, and autoimmune diseases such as lupus, rheumatoid arthritis, and autoimmune thyroid disorders are more common among relatives of people with lupus than the general population. Some scientists believe that the immune system in lupus is more easily stimulated by external factors like viruses or ultraviolet light. Sometimes, symptoms of lupus can be precipitated or aggravated by only a brief period of sun exposure.
It also is known that some women with SLE can experience worsening of their symptoms prior to their menstrual periods. This phenomenon, together with the female predominance of SLE, suggests that female hormones play an important role in the expression of SLE. This hormonal relationship is an active area of ongoing study by scientists.
More recently, research has demonstrated evidence that a key enzyme's failure to dispose of dying cells may contribute the development of SLE. The enzyme, DNase1, normally eliminates what is called "garbage DNA" and other cellular debris by chopping them into tiny fragments for easier disposal. Researchers turned off the DNase1 gene in mice. The mice appeared healthy at birth, but after six to eight months, the majority of mice without DNase1 showed signs of SLE. Thus, a genetic mutation in a gene that could disrupt the body's cellular waste disposal may be involved in the initiation of SLE.
What are the symptoms and signs of lupus?
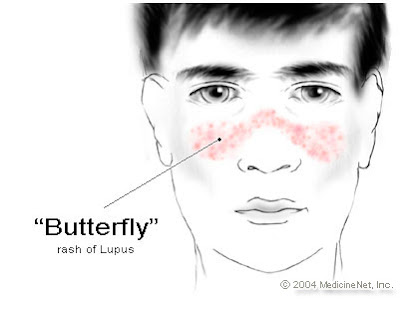
People with SLE can develop different combinations of symptoms and organ involvement. Common complaints and symptoms include fatigue, low-grade fever, loss of appetite, muscle aches, arthritis, ulcers of the mouth and nose, facial rash ("butterfly rash"), unusual sensitivity to sunlight (photosensitivity), inflammation of the lining that surrounds the lungs (pleuritis) and the heart (pericarditis), and poor circulation to the fingers and toes with cold exposure (Raynaud's phenomenon). Complications of organ involvement can lead to further symptoms that depend on the organ affected and severity of the disease.
Skin manifestations are frequent in lupus and can sometimes lead to scarring. In discoid lupus, only the skin is typically involved. The skin rash in discoid lupus often is found on the face and scalp. It usually is red and may have raised borders. Discoid lupus rashes are usually painless and do not itch, but scarring can cause permanent hair loss (alopecia). Over time, 5%-10% of those with discoid lupus may develop SLE.
Over half of the people with SLE develop a characteristic red, flat facial rash over the bridge of their nose. Because of its shape, it is frequently referred to as the "butterfly rash" of SLE. The rash is painless and does not itch. The facial rash, along with inflammation in other organs, can be precipitated or worsened by exposure to sunlight, a condition called photosensitivity. This photosensitivity can be accompanied by worsening of inflammation throughout the body, called a "flare" of the disease.
Typically, with treatment, this rash can heal without permanent scarring.
Most people with SLE will develop arthritis during the course of their illness. Arthritis in SLE commonly involves swelling, pain, stiffness, and even deformity of the small joints of the hands, wrists, and feet. Sometimes, the arthritis of SLE can mimic that of rheumatoid arthritis (another autoimmune disease).
More serious organ involvement with inflammation occurs in the brain, liver, and kidneys. White blood cells and blood-clotting factors also can be characteristically decreased in SLE, known as leukopenia (leucopenia) and thrombocytopenia, respectively. Leukopenia can increase the risk of infection and thrombocytopenia can increase the risk of bleeding.
Inflammation of muscles (myositis) can cause muscle pain and weakness. This can lead to elevations of muscle enzyme levels in the blood.
Inflammation of blood vessels (vasculitis) that supply oxygen to tissues can cause isolated injury to a nerve, the skin, or an internal organ. The blood vessels are composed of arteries that pass oxygen-rich blood to the tissues of the body and veins that return oxygen-depleted blood from the tissues to the lungs. Vasculitis is characterized by inflammation with damage to the walls of various blood vessels. The damage blocks the circulation of blood through the vessels and can cause injury to the tissues that are supplied with oxygen by these vessels.
Inflammation of the lining of the lungs (pleuritis) and of the heart (pericarditis) can cause sharp chest pain. The chest pain is aggravated by coughing, deep breathing, and certain changes in body position. The heart muscle itself rarely can become inflamed (carditis). It has also been shown that young women with SLE have a significantly increased risk of heart attacks due to coronary artery disease.
Kidney inflammation in SLE can cause leakage of protein into the urine, fluid retention, high blood pressure, and even kidney failure. This can lead to further fatigue and swelling of the legs and feet. With kidney failure, machines are needed to cleanse the blood of accumulated waste products in a process called dialysis.
Involvement of the brain can cause personality changes, thought disorders (psychosis), seizures, and even coma. Damage to nerves can cause numbness, tingling, and weakness of the involved body parts or extremities. Brain involvement is referred to as lupus cerebritis.
Many people with SLE experience hair loss (alopecia). Often, this occurs simultaneously with an increase in the activity of their disease. The hair loss can be patchy or diffuse and appear to be more like hair thinning.
Some people with SLE have Raynaud's phenomenon. In this condition, the blood supply to the fingers and/or toes becomes compromised upon exposure to cold, causing blanching, whitish and/or bluish discoloration, and pain and numbness in the exposed fingers and toes.
How is lupus diagnosed?
Since individuals with SLE can have a wide variety of symptoms and different combinations of organ involvement, no single test establishes the diagnosis of systemic lupus. To help doctors improve the accuracy of the diagnosis of SLE, 11 criteria were established by the American Rheumatism Association. These 11 criteria are closely related to the symptoms discussed above. Some people suspected of having SLE may never develop enough criteria for a definite diagnosis. Other people accumulate enough criteria only after months or years of observation. When a person has four or more of these criteria, the diagnosis of SLE is strongly suggested. Nevertheless, the diagnosis of SLE may be made in some settings in people with only a few of these classical criteria, and treatment may sometimes be instituted at this stage. Of these people with minimal criteria, some may later develop other criteria, but many never do.
The 11 criteria used for diagnosing systemic lupus erythematosus are
•malar (over the cheeks of the face) "butterfly" rash,
•discoid skin rash (patchy redness with hyperpigmentation and hypopigmentation that can cause scarring),
•photosensitivity (skin rash in reaction to sunlight [ultraviolet light] exposure),
•mucous membrane ulcers (spontaneous ulcers of the lining of the mouth, nose, or throat),
•arthritis (two or more swollen, tender joints of the extremities),
•pleuritis or pericarditis (inflammation of the lining tissue around the heart or lungs, usually associated with chest pain upon breathing or changes of body position),
•kidney abnormalities (abnormal amounts of urine protein or clumps of cellular elements called casts detectable with a urinalysis),
•brain irritation (manifested by seizures [convulsions] and/or psychosis),
•blood-count abnormalities (low counts of white or red blood cells, or platelets, on routine blood testing),
•immunologic disorder (abnormal immune tests include anti-DNA or anti-Sm [Smith] antibodies, falsely positive blood test for syphilis, anticardiolipin antibodies, lupus anticoagulant, or positive LE prep test),
•antinuclear antibody (positive ANA antibody testing [antinuclear antibodies
What is the treatment for systemic lupus erythematosus?
There is no permanent cure for SLE. The goal of treatment is to relieve symptoms and protect organs by decreasing inflammation and/or the level of autoimmune activity in the body. Many people with mild symptoms may need no treatment or only intermittent courses of anti-inflammatory medications. Those with more serious illness involving damage to internal organ(s) may require high doses of corticosteroids in combination with other medications that suppress the body's immune system.
People with SLE need more rest during periods of active disease. Researchers have reported that poor sleep quality was a significant factor in developing fatigue in people with SLE. These reports emphasize the importance for people and physicians to address sleep quality and the effect of underlying depression, lack of exercise, and self-care coping strategies on overall health. During these periods, carefully prescribed exercise is still important to maintain muscle tone and range of motion in the joints.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are helpful in reducing inflammation and pain in muscles, joints, and other tissues. Examples of NSAIDs include aspirin, ibuprofen (Motrin), naproxen (Naprosyn), and sulindac (Clinoril). Since the individual response to NSAIDs varies, it is common for a doctor to try different NSAIDs to find the most effective one with the fewest side effects. The most common side effects are stomach upset, abdominal pain, ulcers, and even ulcer bleeding. NSAIDs are usually taken with food to reduce side effects. Sometimes, medications that prevent ulcers while taking NSAIDs, such as misoprostol (Cytotec), are given simultaneously.
Corticosteroids are more potent than NSAIDs in reducing inflammation and restoring function when the disease is active. Corticosteroids are particularly helpful when internal organs are affected. Corticosteroids can be given by mouth, injected directly into the joints and other tissues, or administered intravenously. Unfortunately, corticosteroids have serious side effects when given in high doses over prolonged periods, and the doctor will try to monitor the activity of the disease in order to use the lowest doses that are safe. Side effects of corticosteroids include weight gain, thinning of the bones and skin, infection, diabetes, facial puffiness, cataracts, and death (necrosis) of the tissues in large joints.
Hydroxychloroquine (Plaquenil) is an antimalarial medication found to be particularly effective for SLE people with fatigue, skin involvement, and joint disease. Consistently taking Plaquenil can prevent flare-ups of lupus. Side effects are uncommon but include diarrhea, upset stomach, and eye-pigment changes. Eye-pigment changes are rare but require monitoring by an ophthalmologist (eye specialist) during treatment with Plaquenil. Researchers have found that Plaquenil significantly decreased the frequency of abnormal blood clots in people with systemic lupus. Moreover, the effect seemed independent of immune suppression, implying that Plaquenil can directly act to prevent the blood clots. This fascinating study highlights an important reason for people and doctors to consider Plaquenil for long-term use, especially for those SLE people who are at some risk for blood clots in veins and arteries, such as those with phospholipid antibodies (cardiolipin antibodies, lupus anticoagulant, and false-positive venereal disease research laboratory test). This means not only that Plaquenil reduces the chance for re-flares of SLE, but it can also be beneficial in thinning the blood to prevent abnormal excessive blood clotting. Plaquenil is commonly used in combination with other treatments for lupus.
For resistant skin disease, other antimalarial drugs, such as chloroquine (Aralen) or quinacrine, are considered and can be used in combination with hydroxychloroquine. Alternative medications for skin disease include dapsone and retinoic acid (Retin-A). Retin-A is often effective for an uncommon wart-like form of lupus skin disease. For more severe skin disease, immunosuppressive medications are considered as described below.
Medications that suppress immunity (immunosuppressive medications) are also called cytotoxic drugs. Immunosuppressive medications are used for treating people with more severe manifestations of SLE, such as damage to internal organ(s). Examples of immunosuppressive medications include methotrexate (Rheumatrex, Trexall), azathioprine (Imuran), cyclophosphamide (Cytoxan), chlorambucil (Leukeran), and cyclosporine (Sandimmune). All immunosuppressive medications can seriously depress blood-cell counts and increase risks of infection and bleeding. Other side effects are specific for each drug. For examples, Rheumatrex can cause liver toxicity, while Sandimmune can impair kidney function.
In recent years, mycophenolate mofetil (CellCept) has been used as an effective medication for lupus, particularly when it is associated with kidney disease. CellCept has been helpful in reversing active lupus kidney disease (lupus renal disease) and in maintaining remission after it is established. Its lower side-effect profile has advantage over traditional immune-suppression medications.
In SLE patients with serious brain or kidney disease, plasmapheresis (a process of removing and treating the blood before it is returned to the body) is sometimes used to remove antibodies and other immune substances from the blood to suppress immunity. Rarely, people with SLE can develop seriously low platelet levels, thereby increasing the risk of excessive and spontaneous bleeding. Since the spleen is believed to be the major site of platelet destruction, surgical removal of the spleen is sometimes performed to improve platelet levels. Other treatments have included plasmapheresis and the use of male hormones. Plasmapheresis has also been used to remove proteins (cryoglobulins) that can lead to vasculitis. End-stage kidney damage from SLE requires dialysis and/or a kidney transplant.
Most recent research is indicating benefits of rituximab (Rituxan) in treating lupus. Rituximab is an intravenously infused antibody that suppresses a particular white blood cell, the B cell, by decreasing their number in the circulation. B cells have been found to play a central role in lupus activity, and when they are suppressed, the disease tends toward remission. This may particularly helpful for people with kidney disease.
Scientists have also found that low-dose dietary supplementation with omega-3 fish oils could help patients with lupus by decreasing disease activity and possibly decreasing heart-disease risk.
How can a lupus patient help prevent disease activity (flares)?
SLE is undoubtedly a potentially serious illness with involvement of numerous organ systems. However, it is important to recognize that most people with SLE lead full, active, and healthy lives. Periodic increases in disease activity (flares) can usually be managed by varying medications. Since ultraviolet light can precipitate and worsen flares, people with systemic lupus should avoid sun exposure. Sunscreens and clothing covering the extremities can be helpful. Abruptly stopping medications, especially corticosteroids, can also cause flares and should be avoided. People with SLE are at increased risk of infections, especially if they are taking corticosteroids or immunosuppressive medications. Therefore, any unexpected fever should be reported and evaluated.
The key to successful management of SLE is regular contact and communication with the doctor, allowing monitoring of symptoms, disease activities, and treatment of side effects.
How can systemic lupus erythematosus affect pregnancy or the newborn?
Women with SLE who become pregnant are considered "high risk." Women with SLE who are pregnant require close observation during pregnancy, delivery, and the postpartum period. This includes fetal monitoring by the obstetrician during later pregnancy. These women can have an increased risk of miscarriages (spontaneous abortions) and can have flares of SLE during pregnancy. The presence of phospholipid antibodies, such as cardiolipin antibodies or lupus anticoagulant, in the blood can identify people at risk for miscarriages. Cardiolipin antibodies are associated with a tendency toward blood clotting. People with SLE who have cardiolipin antibodies or lupus anticoagulant may need blood-thinning medications (aspirin with or without heparin) during pregnancy to prevent miscarriages. Other reported treatments include the use of intravenous gamma globulin for selected people with histories of premature miscarriage and those with low blood-clotting elements (platelets) during pregnancy. Pregnant women who have had a previous blood-clotting event may benefit by continuation of blood-thinning medications throughout and after pregnancy for up to six to 12 weeks, at which time the risk of clotting associated with pregnancy seems to diminish. Plaquenil has now been found to be safe for use to treat SLE during pregnancy.
Lupus antibodies can be transferred from the mother to the fetus and result in lupus illness in the newborn ("neonatal lupus"). This includes the development of low red cell (anemia) and/or white blood cell and platelet counts, and skin rash. Problems can also develop in the electrical system of the baby's heart (congenital heart block). Occasionally, a pacemaker for the baby's heart is needed in this setting. Neonatal lupus and congenital heart block are more common in newborns of mothers with SLE who carry antibodies referred to as anti-Ro (or SS-A) and anti-La (or SS-B). (It is wise for the newborn baby's doctor to be made aware if the mother is known to carry these antibodies, even prior to delivery. The risk of heart block is 2%; the risk of neonatal lupus is 5%.) Neonatal lupus usually clears after 6 months of age, as the mother's antibodies are slowly metabolized by the baby.
Untuk maklumat lebih lanjut.. sila layari http://www.medicinenet.com/systemic_lupus/article.htm
So..to all my friend..please take care of yourself..please go to hospital when u feel not confortable or sick..love urself..its a must!

{kind=link}